Types of Head and Neck Cancer
Salivary Gland Cancer
On this page
Head&Neck Cancer Types
Cancer Description
The salivary glands make spit (saliva) and release saliva to keep the mouth and throat moist and help with swallowing and digesting food. There are 3 major (large) and over 600 minor (small) salivary glands.
Tumours of the salivary glands can be benign (not cancer) or malignant (cancer).
The 3 pairs of major salivary glands include: the Parotid Gland, Submandibular glands and Sublingual glands.
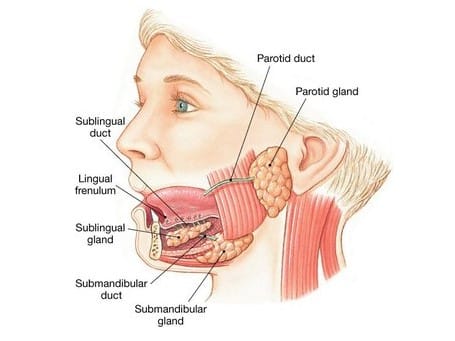
- Parotid Glands – are found just in front of the ears and behind the jaw. They move saliva into the mouth through a tube called the parotid duct. This tube opens on the inside of the cheek, near the upper molar teeth. The parotid gland is the largest salivary gland and most salivary tumours start here.
- Submandibular Glands – lie under the jawbone, one on each side. They release saliva into the mouth through a duct (tube) that opens in the floor of the mouth, under the tip of the tongue.
- Sublingual Glands – lie under the tongue, one on each side. They release saliva into the submandibular duct and are near the lingual nerves which give feeling and taste to the front of the tongue. The sublingual glands are the smallest of the major salivary glands.
- Minor Salivary Glands – There are hundreds of minor salivary glands throughout the mouth and throat. They can be found inside the mouth, just under the surface including the lips, cheeks and top of the mouth (soft palate).
Rarity and complexity of salivary gland cancers
Salivary gland cancers are very rare, with about 500 diagnoses per year in the UK. There are approximately 25 different types of salivary gland cancers. The rarity makes diagnosis and treatment challenging, as most doctors will only encounter a small number of cases in their professional experience.
The most common types of Salivary Gland cancers are:
- Mucoepidermoid carcinomas. Mostly common in the parotid glands.
- Two types of cancer are abbreviated as ACC so it is important to use the full name to avoid confusion:
- Adenoid Cystic Carcinoma (more aggressive). Sometimes it can form in other parts of the body, including your skin, breast tissue, cervix or prostate gland.
- Acinic Cell Carcinoma (less aggressive). Acinic Cell Carcinoma (AciCC) is a relatively rare, low-grade malignant tumor that most commonly occurs in the parotid gland. It typically grows slowly and represents about 10-15% of all malignant salivary gland tumours.
Symptoms of salivary gland cancer
The main symptoms of salivary gland cancer is a lump or swelling in one of the glands on or near your jaw, or in your mouth or neck. These lumps tend to be tender or give shooting pains. Other symptoms can include numbness in part of your face and drooping on one side of your face.
Symptoms of Adenoid Cystic Carcinoma
These include headaches and seizures but much depends on the tumour’s location. The primary sign is a lump in the salivary gland areas; in front of the ears (parotid glands), in the neck, inside the mouth (minor salivary glands in lips, cheeks, or roof of the mouth) and may cause painless masses in the mouth or face. Tumours of the lacrimal gland (small almond-shaped structure that secretes tears and is located just above the upper, outer corner of each eye) cause a bulging eye or changes in vision. Those situated in the windpipe or voice box may cause respiratory symptoms or changes in speech.
Other Adenoid Cystic Carcinoma specific symptoms also include; numbness or a pins and needles sensation, weakness in facial muscles and pain (can occur earlier than in other types due to nerve involvement).
Common Treatment Approaches
The treatment for salivary gland cancer typically involves a combination of treatment methods, and the exact prognosis depends heavily on the stage at diagnosis. Your consultant will describe your specific treatment and prognosis. The information below is for illustration purposes only;
- Surgery. This is primary treatment for most salivary gland cancers. It involves removing the affected gland and possibly surrounding tissue and may include lymph node removal if cancer has spread. Much depends on the stage and size of the affected area, laser surgery can be used to accurately removal the tumour.
- Radiotherapy. Often used after surgery to kill remaining cancer cells. Sometimes used as primary treatment if surgery isn’t possible and may be given before surgery in some cases to shrink the tumour. The treatment may be combined with chemotherapy (chemoradiation).
- Chemotherapy. Less commonly used than surgery or radiation. May be recommended for advanced cases.
Your consultant will evaluate your overall general health at the point of diagnosis looking at the following aspects; the cancer stage at diagnosis, age and lifestyle.
The consultant will have regular check-ups with you for at least 5 years after treatment. Many patients can return to normal activities, though some may experience lasting effects from treatment, such as dry mouth or changes in swallowing function. See Post Treatment side effects.
Adenoid Cystic Carcinoma Information
Adenoid Cystic Carcinoma is a rare form of adenocarcinoma, a type of cancer that begins in glandular tissues (a group of cells that produce and release substances such as hormones into the bloodstream). Adenoid Cystic Carcinoma arises within glands most commonly in the major and minor salivary glands of the head and neck. It is a more aggressive type of salivary gland cancer and tends to spread earlier and through nerves. It often requires multi-modality treatment and has a high rate of recurrence.
Adenoid Cystic Carcinoma accounts for about 1% of all cases of head and neck cancer. It is more prevalent in women, accounting for nearly two thirds of all new cases diagnosed.
The cause of Adenoid Cystic Carcinoma is currently unknown, however it does not appear to run in families. There is evidence that it likely develops from genetic changes that occur over the patient’s lifetime, and, although the changes may be caused by environmental exposures, there are no strong environmental risk factors for Adenoid Cystic Carcinoma that have been identified to date. The genetic mutations are only present in the cancer cells, and not in the egg and sperm cells which are passed on to the next generation.
Contrary to other head and neck cancers, lifestyle choices such as smoking or alcohol use are not linked to increased risk of Adenoid Cystic Carcinoma. Infection by the human papilloma virus (HPV) also does not seem to increase risk.
Diagnosis and Treatment of Adenoid Cystic Carcinoma
Early diagnosis is crucial for this aggressive form of salivary gland cancer. Any persistent lump (lasting more than 3 weeks) should be investigated. Treatment is managed by head and neck cancer specialists using a range of techniques. Research and Data Collection is to aid ongoing efforts to improve treatments and experience sharing among specialist clinicians. Patients are encouraged to participate in data registries and audits to advance understanding and treatment of these rare cancers
Note for Patients: while salivary gland cancers are rare, being aware of the signs and symptoms can aid in early detection. If you notice any persistent lumps or unusual symptoms in the head and neck area, consult your healthcare provider promptly.
Useful links
Suggested additional sites that may offer helpful information:
Patient Stories





Please join our private Facebook Group to get support and advice from fellow patients and carers

Oracle Head & Neck Cancer UK is a registered charity in England and Wales (1142037), and in Scotland (SC052790).
Registered as a company limited by guarantee in England and Wales (7125497). Registered address: 167-169, Great Portland Street, 5th Floor, London W1W 5PF.