Types of Head and Neck Cancer
Mouth Cancer
On this page
Head&Neck Cancer Types
Cancer Description
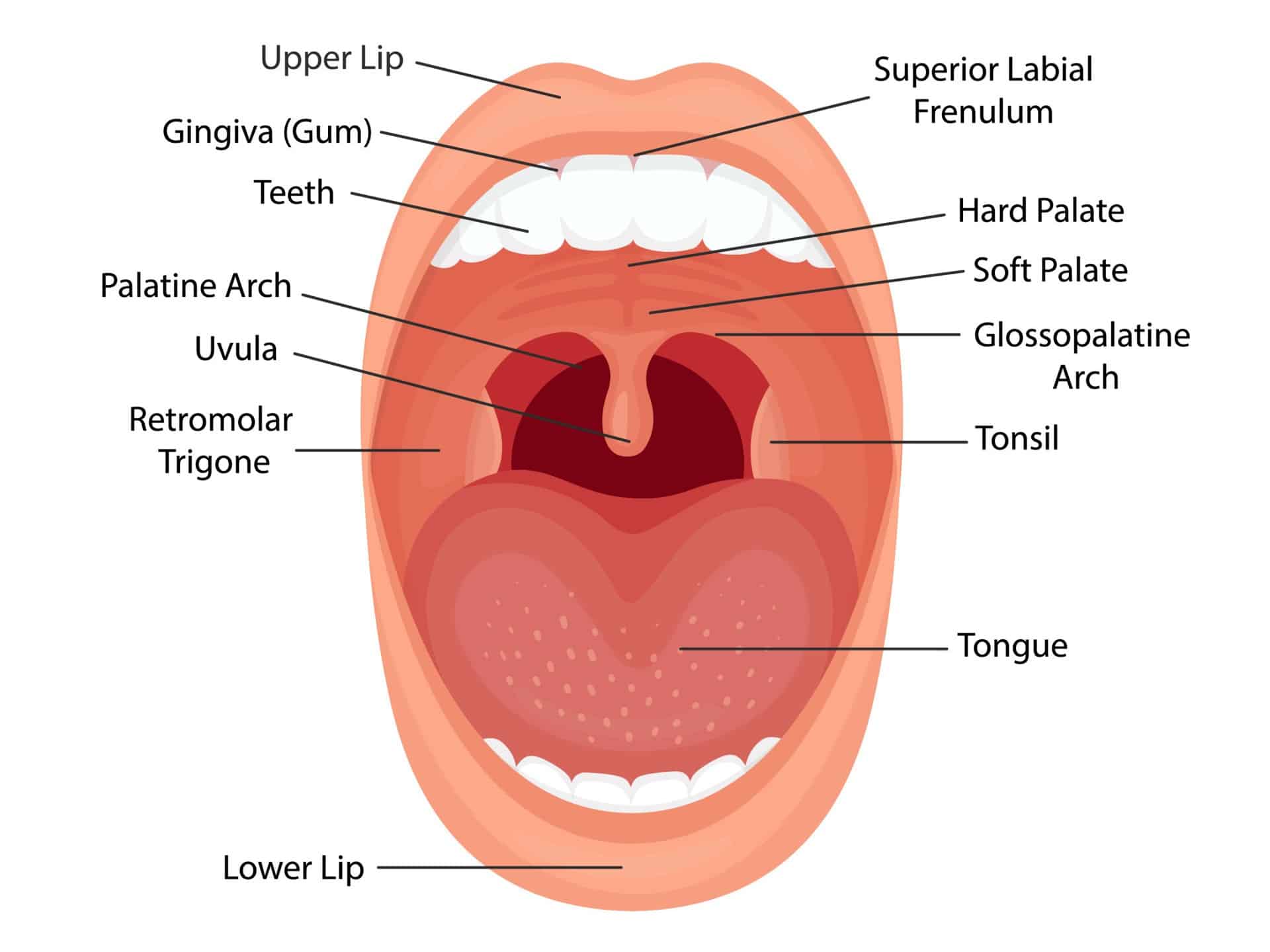
The oral cavity includes the mouth and tongue. Mouth cancer can affect a number of areas in and around the mouth, including the:
- lips
- tongue
- inside of the cheeks
- floor or roof of the mouth, under the tongue
- area behind the wisdom teeth
- gums and the jaw
Primary causes of mouth or oral cancers are through tobacco use (smoking or chewing), heavy alcohol consumption and combined tobacco and alcohol use significantly increases the risks.
There is strong link with the human papilloma virus (HPV). Prolonged sun exposure, particularly for lip cancer and family history are recognised risk factors. Poor oral hygiene and poor diet that is lacking in fruits and vegetables are less well proven risk factors.
Symptoms of mouth cancer
Symptoms of cancers within the mouth can include:
- mouth ulcers or sores that last 3 weeks or longer and unexplained,
- persistent lumps in your mouth, lip or jaw area, which may or may not be painful.
- bad breath (halitosis)
- red patches (erythroplakia) or white patches (leukoplakia)
- an ear ache that does not go away
- unexplained bleeding
- difficulty swallowing
Common Treatment Approaches
The treatment for mouth cancer typically involves a combination of treatment methods, and the exact prognosis depends heavily on the stage at diagnosis and whether the cancer is HPV-positive or negative. The biopsy will provide the necessary information on whether the tumour is HPV-positive or negative. Your consultant will describe your specific treatment and prognosis. The information below is for illustration purposes only;
- Surgery. In tongue surgery the term glossectomy is used. A “partial” glossectomy is the removal of less than half of the tongue. A hemiglossectomy is when approximately half of the tongue is removed and a total/subtotal glossectomy is where nearly all the tongue is removed. Everybody will be different, but clearly, the size and location of the tumour will dictate whether or the tongue needs to be reconstructed. Surgery may be combined with radiotherapy to give a “safety margin” around the tumour site.
- Radiotherapy. Often a primary treatment, usually 30 to 35 doses are given over 5 days a week for 6-7 weeks. The treatment may be combined with chemotherapy (chemoradiation). Modern techniques like IMRT (Intensity-Modulated Radiation Therapy) help minimize side effects in the future.
- Chemotherapy. Usually combined with radiotherapy and may be given before, during, or after radiotherapy. Often the secondary treatment, usually 3 cycles of chemo are given at the beginning, middle and end of the radiotherapy calendar. Common drugs used include cisplatin, carboplatin, and 5-fluorouracil.
The prognosis for HPV-positive cancer is generally better than HPV-negative cancer. The 5-year survival rate for HPV-positive cancer is 80-90% combined with 50-60% for HPV-negative cancer. The latter is often related to smoking/alcohol use and has a higher risk of recurrence. Your consultant will evaluate your overall general health at the point of diagnosis looking at the following aspects; the cancer stage at diagnosis, age and lifestyle.
The consultant will have regular check-ups with you for at least 5 years after treatment. Many patients can return to normal activities, though some may experience lasting effects from treatment, such as dry mouth or changes in swallowing function. See Post Treatment side effects.
Useful Links
Suggested additional sites that may offer helpful information:
Mouth cancer tests and next steps in the NHS
Mouth cancer foundation referral advice
Podcasts
This podcast gives the latest Mouth cancer figures and HPV relationship. The latest figures are out and they don´t look good.
This oral health podcast is dedicated to HPV vaccine podcast. People are not having the HPV vaccine, so what impact is that having on mouth cancer incidence rates?
Patient Stories










Please join our private Facebook Group to get support and advice from fellow patients and carers

Oracle Head & Neck Cancer UK is a registered charity in England and Wales (1142037), and in Scotland (SC052790).
Registered as a company limited by guarantee in England and Wales (7125497). Registered address: 167-169, Great Portland Street, 5th Floor, London W1W 5PF.